What the evidence on dementia prevention actually shows
Most clinical encounters with dementia happen after symptoms have appeared. A fall that turns out to be more than a fall. A memory complaint a family has been quietly managing for years. An infection that lifts to reveal something underneath. Some patients are caught earlier, at mild cognitive impairment, in the workup of someone made watchful by family history. But most dementia, when clinicians meet it, has already announced itself. By then the window for the highest-leverage prevention has substantially narrowed.
That is the dementia most physicians know. It is not the stage where prevention does its work.
The work happens decades earlier, in the period when the brain is changing but the person is not yet symptomatic. For most of the past twenty years, the honest answer about what to do during that window was "we are not sure." That answer has begun to change. The first major positive prevention trial, FINGER, was published in 2015, and most of what now constitutes the evidence base has accumulated since then, through SPRINT MIND, the ACHIEVE hearing trial, the long-term ACTIVE results, US POINTER, and two Lancet Commission updates. The field has shifted, quietly enough that most people, including most physicians, have not yet absorbed how much the picture has changed.
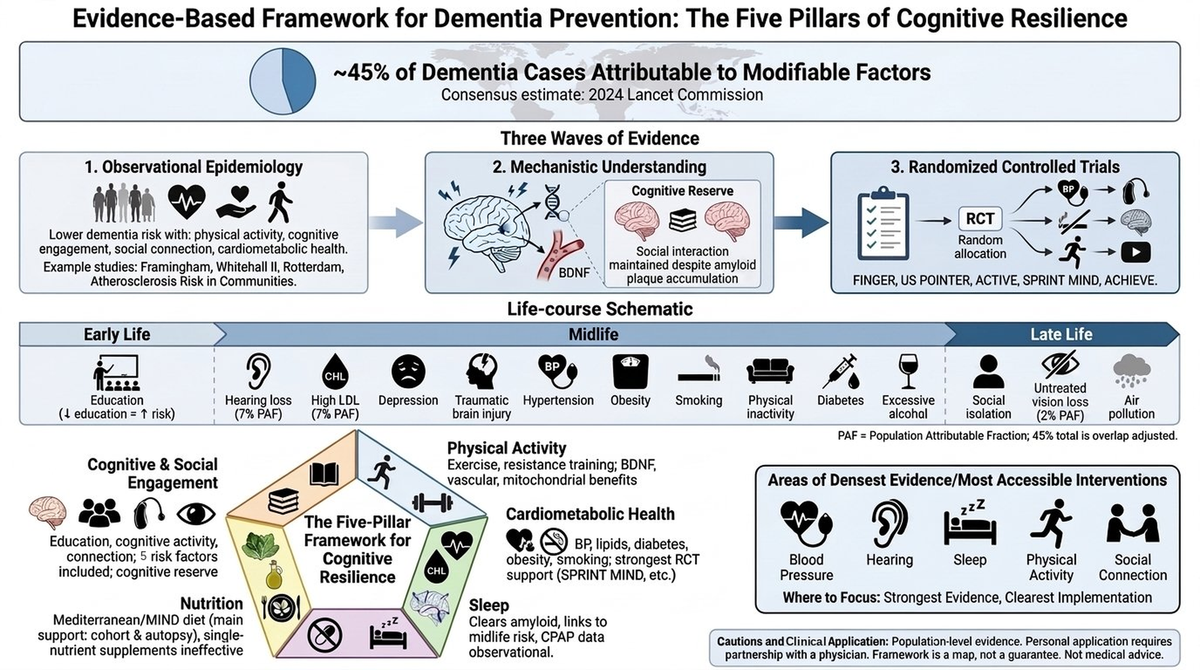
The Lancet Commission on dementia estimates that around 45 percent of dementia cases worldwide are associated with factors that can, in principle, be modified.
That figure comes from the most authoritative synthesis in the field, updated in 2024. It is not a fringe estimate; it is the consensus position of an international panel reviewing the entire body of evidence. Almost half. It also rests heavily on observational data, so it describes an association across populations, not a guaranteed return on any individual's effort, a distinction this series will keep returning to.
You might expect that number to anchor every conversation about brain health. It does not. The public discourse oscillates between fatalism and hype. The fatalist position is that nothing really works and it is mostly genetic. The hype position is this supplement, this app, this hack. Neither matches what the research shows, and the result is a population that hears too much noise and has little sense of what the evidence actually supports.
Cognitive Resilience is built to address that. The premise is simple. There is now enough high-quality research on brain health to make the case clearly, take positions where the data support them, and acknowledge the gaps honestly where they do not. No supplements to sell. No hacks. Just a synthesis of what the evidence shows, written for adults who want to engage with the research rather than the headlines.
The trajectory matters
The first thing to understand is that brain health is not a hypothetical future intervention. It is happening, in aggregate, right now.
Dementia incidence has fallen in high-income countries over the past three decades, even as the total number of people with dementia rises because populations are aging. Age-adjusted incidence rates are dropping. The pattern shows up in the Framingham Heart Study, in European cohorts, and in US population surveys, and it tracks with better education, better blood pressure control, better cardiovascular care, and reductions in smoking.
This matters because it speaks to the most common objection to dementia prevention, that we do not really know whether any of it works. At the population level, the trend is real, and the factors associated with it are the same ones the evidence base supports for individuals. The open question is less whether modifiable factors matter and more how to translate what is working at the population level into the choices an individual can make.
The trajectory exists. The question is who gets to participate in it.
Three waves of evidence
The case for cognitive resilience rests on three increasingly strong waves of evidence, and understanding that layered structure is key to evaluating any specific claim in this field.
The first wave is observational epidemiology. For decades, cohort studies have tracked thousands of people across thirty or more years of follow-up, and the pattern is consistent across cohorts that span continents, demographics, and definitions. Physically active, cognitively engaged, socially connected, cardiometabolically healthy adults develop dementia at lower rates. Whitehall II, Framingham, the Rush Memory and Aging Project, the Honolulu-Asia Aging Study, the Rotterdam Study, and the Atherosclerosis Risk in Communities study reach the same answer through different populations and methods. The recurring caution, the one this publication's exercise work examines in depth, is that observational patterns can be shaped by reverse causation, where early, undiagnosed disease alters behavior years before diagnosis.
The second wave is mechanism. Why would these associations exist? Autopsy data show that highly educated, physically active, socially engaged individuals develop less clinical impairment at any given level of brain pathology. Two people can carry the same burden of amyloid and tau at death and have lived very different cognitive lives. The neurologist Yaakov Stern formalized this as cognitive reserve, a buffer between biological brain damage and functional decline. Exercise stimulates BDNF and supports cerebral blood flow. Sleep may help clear amyloid and other metabolic waste, partly through a glymphatic pathway described in the last decade, though how much of that work depends on sleep in humans is still being worked out. Cardiometabolic health protects the small vessels that supply the brain. And dietary patterns, according to autopsy work from Rush published in 2023, may even be associated with less Alzheimer's pathology itself. The mechanism story is strong even where the trial evidence is incomplete.
The third wave is randomized trials, and this is where the field has matured fastest in the past decade. FINGER, in Finland in 2015, was the first major multidomain prevention trial to show cognitive benefit in at-risk older adults. US POINTER, in 2025, reproduced that signal in an American population. ACHIEVE, in 2023, tested hearing intervention with cognitive endpoints; the primary outcome was not significant in the full cohort, but in a prespecified higher-risk subgroup the intervention slowed cognitive decline by roughly half. SPRINT MIND showed that intensive blood pressure control significantly reduced mild cognitive impairment, with the dementia-only endpoint trending the same way without reaching significance. And the ACTIVE trial's speed-of-processing training was associated with lower dementia incidence at ten years, about 29 percent, though that result sat at the edge of statistical significance, was not significant at five years, fell on a secondary endpoint, and the authors themselves called for replication. These are large, multi-year, randomized trials with cognitive endpoints, and most have appeared in the last decade, but they vary in strength, and reading them honestly means saying so.
Three waves of evidence, pointing the same direction with different degrees of confidence.
The fourteen factors, and what they mean
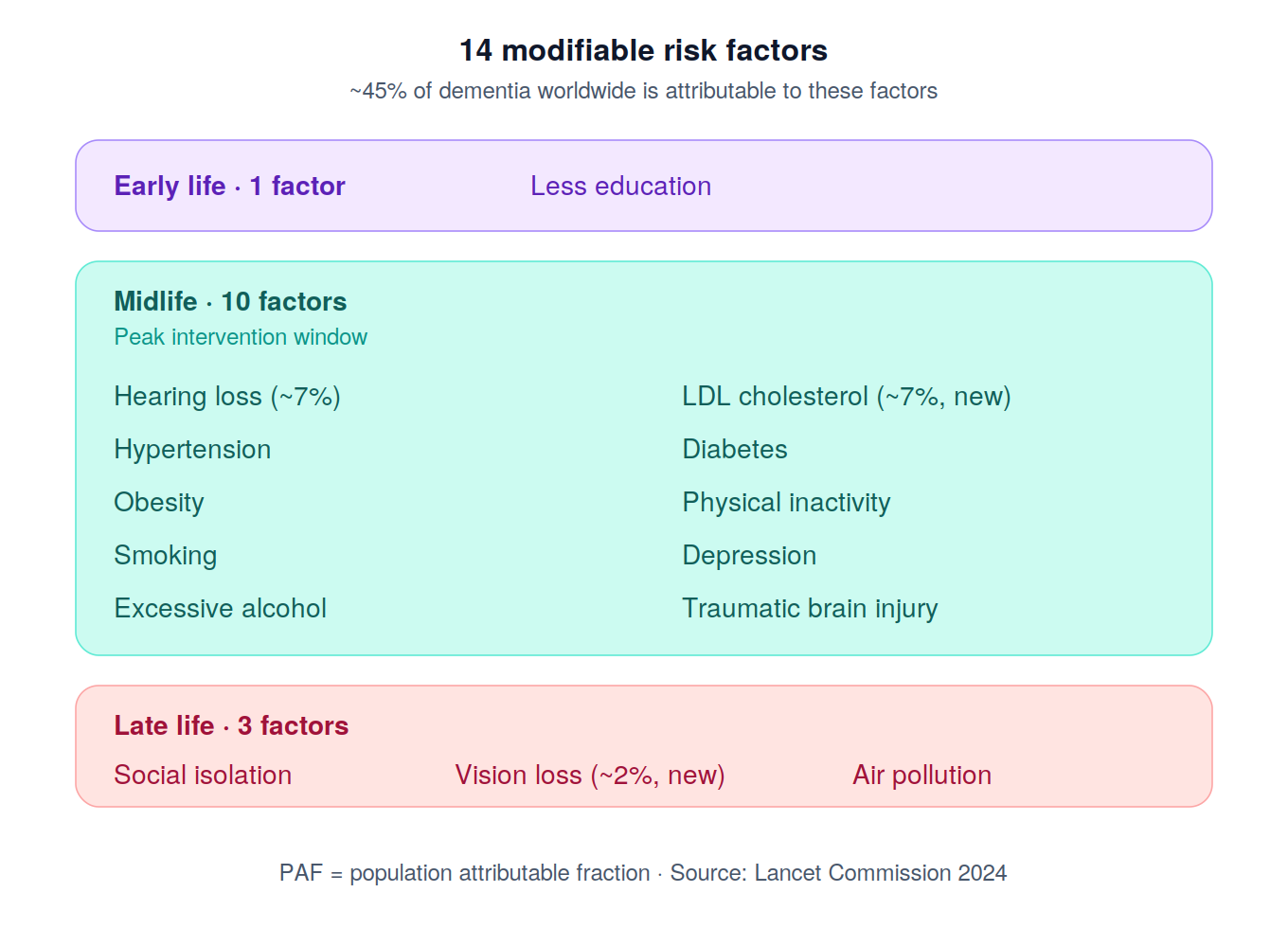
The Lancet Commission organizes the modifiable risk factors across the life course. Around 45 percent of dementia cases worldwide are associated with fourteen of them.
In early life, less education. In midlife, hearing loss, high LDL cholesterol, depression, traumatic brain injury, hypertension, obesity, smoking, physical inactivity, diabetes, and excessive alcohol. In late life, social isolation, untreated vision loss, and air pollution.
Hearing loss is the single largest midlife factor. High LDL cholesterol was newly added in 2024 with similar weight. The cardiometabolic cluster, covering hypertension, diabetes, obesity, LDL, physical inactivity, and smoking, collectively accounts for a substantial share of the preventable burden.
These percentages are weighted population attributable fractions calculated from cohort data. They are not promises. Each represents the proportional reduction in dementia cases that would occur if a given risk factor were eliminated from the population, and the 45 percent total is adjusted for overlap between factors. The framework describes population epidemiology, not individual destiny, and because it is built on observational data, it carries the same interpretive caution as the first wave above.
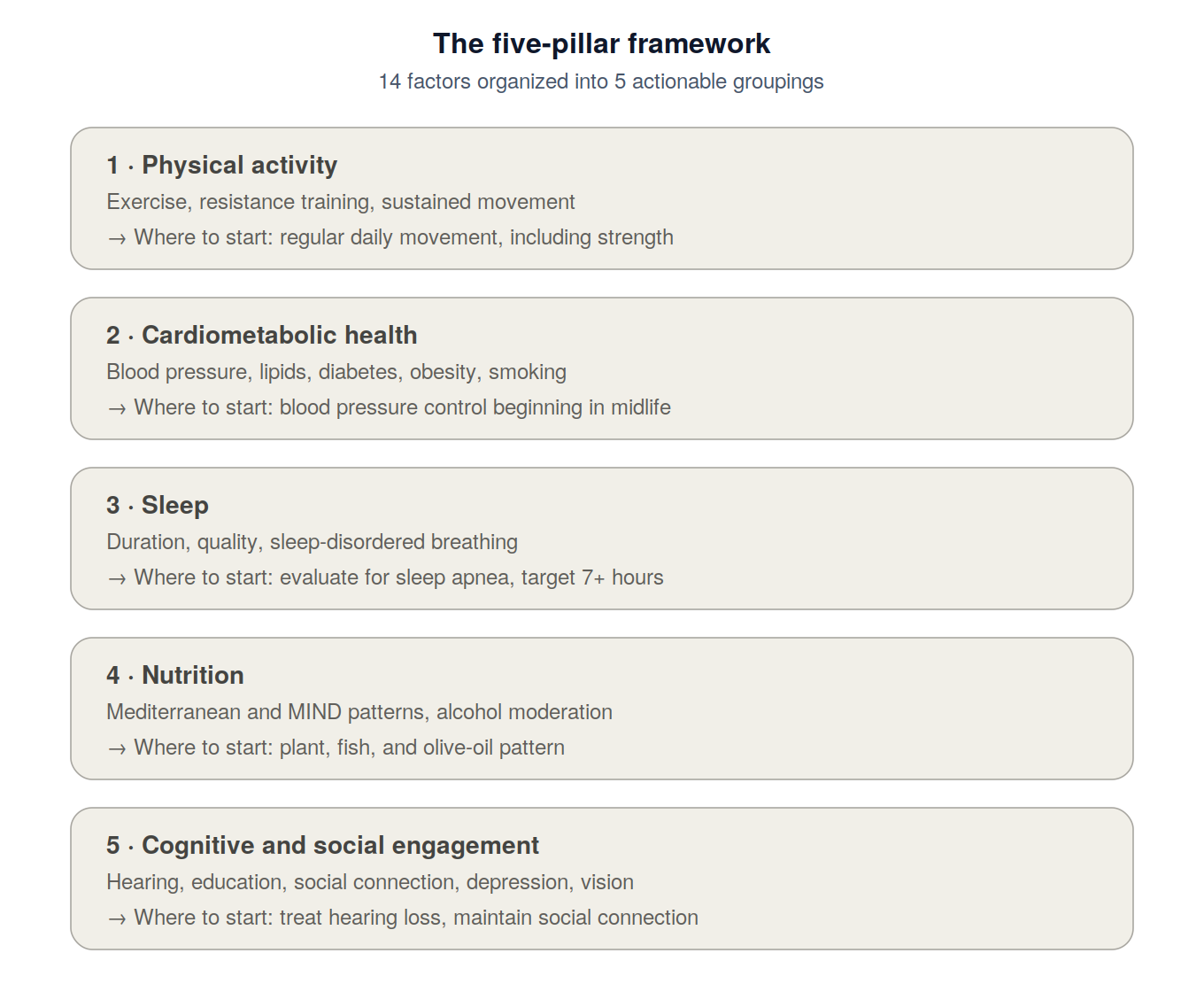
The five-pillar framework
Fourteen factors is too many for any individual to operationalize. Cognitive Resilience uses a five-pillar framework that collapses them into actionable groupings, each gathering factors that share a mechanism.
Physical activity covers exercise, structured movement, and resistance training. The observational signal is rich, and the mechanisms, BDNF, vascular function, mitochondrial health, are well grounded. The 2011 finding that aerobic exercise expanded hippocampal volume has not consistently replicated in healthy older adults, but progressive resistance training in people with mild cognitive impairment has shown a structural brain benefit. This is the pillar where the gap between the popular story and the trial evidence is widest, and the exercise series examines it closely.
Cardiometabolic health covers blood pressure, lipids, diabetes, obesity, and smoking. This cluster has the strongest randomized trial evidence in the entire field: SPRINT MIND on hypertension, the 2024 addition of LDL cholesterol, the diabetes-dementia literature, and substantial Mendelian randomization and epidemiologic support for smoking. Addressed comprehensively, it is probably the single largest individual lever available.
Sleep is not among the Lancet fourteen, but the mechanism story is unusually strong. Sleep appears to support the brain's overnight clearance of metabolic waste, midlife short sleep predicts dementia 25 years later in Whitehall II, and sleep-disordered breathing is a clear independent risk factor, with CPAP treatment associated with delayed cognitive decline in observational data. Sleep belongs in the framework even without a formal attributable fraction, though its causal weight is still being established.
Nutrition has the strangest evidence profile in the field. The Mediterranean and MIND diets carry strong observational support and the strongest autopsy signal of any factor. Yet the MIND diet randomized trial was negative on its primary outcome, and one likely explanation is that both groups lost weight, which raises the possibility that caloric restriction matters as much as specific dietary composition. Single-nutrient supplements have mostly failed in trials, and alcohol is increasingly understood to have no protective threshold for brain health.
Cognitive and social engagement covers education, cognitive activity, social connection, depression, hearing, and vision. The ACHIEVE hearing trial is the cleanest large-trial signal outside the cardiometabolic cluster, and the ACTIVE speed-of-processing finding is the cleanest cognitive-training signal, with the caveats already noted. This pillar is conceptually anchored in cognitive reserve.
What this framework actually tells you
The fourteen factors and five pillars together produce a coherent framework, with several implications.
The case is not equally strong across factors. Cardiometabolic health and hearing intervention have the strongest randomized support. Physical activity and education have the strongest observational and Mendelian randomization support. Sleep and nutrition have rich mechanism stories with developing trial evidence. The framework is layered, not flat, and anyone telling you otherwise, particularly anyone selling a single intervention, is overclaiming.
The factors overlap mechanistically. Treating hypertension protects the brain through the same vascular pathways that physical activity supports. Sleep quality affects metabolic regulation, which affects cardiovascular health. Social engagement supports cognitive activity. The pillars are conceptually distinct but biologically interconnected, which is likely why the multidomain trials show benefit even when individual component trials are mixed.
Life course matters, and the leverage shifts with age. Education operates in early life. Midlife is the highest-yield window for hypertension, hearing, and LDL. Late-life interventions remain meaningful even when earlier factors were not addressed. The framework is a map, not a verdict.
And the evidence is good enough to act on now. Not every factor has a randomized trial, but the convergence of observational evidence across cohorts, mechanistic understanding across systems, and randomized evidence in the highest-leverage areas is strong enough to support a coherent approach. Waiting for a single definitive trial of "the prevention intervention" is not a reasonable strategy, because the disease takes decades to develop, and the interventions need to begin before symptoms appear.
Where the evidence concentrates
For anyone looking at this framework and wondering where to focus before the rest of the series goes deep, five areas stand out as the places the evidence is densest and the interventions most accessible: blood pressure, hearing, sleep, sustained physical activity, and social connection.
These are not the only things that matter. They are where the case is strongest, the trials clearest, and the day-to-day implementation most concrete.
Applying any of this to a real person requires partnership with a physician who knows the individual situation. The framework tells you where the evidence is densest. The personalization is clinical work.
What this series will do
The rest of Cognitive Resilience goes deep on each pillar in turn: what the evidence shows, where the strongest interventions are, where the gaps are, and how the case has evolved.
The trajectory of the field is encouraging in a way that gets very little airtime, because encouraging trajectories do not generate headlines.
If you have been looking for a synthesis that takes the research seriously, takes positions where the evidence supports them, and refuses to either oversell or underdeliver, this publication is built for you.
Cognitive Resilience is written by Atif Hashmi, MD, a board-certified neurologist with fellowship training in neuroimaging. This publication is educational and reflects evolving research synthesis.
References
- Livingston G, Huntley J, Liu KY, et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Lancet. 2024;404(10452):572-628. doi:10.1016/S0140-6736(24)01296-0
- Ngandu T, Lehtisalo J, Solomon A, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial. Lancet. 2015;385(9984):2255-2263. doi:10.1016/S0140-6736(15)60461-5
- Baker LD, Espeland MA, Whitmer RA, et al. Structured vs self-guided multidomain lifestyle interventions for global cognitive function: the US POINTER randomized clinical trial. JAMA. 2025;334(8):681-691. doi:10.1001/jama.2025.12923
- Lin FR, Pike JR, Albert MS, et al. Hearing intervention versus health education control to reduce cognitive decline in older adults with hearing loss in the USA (ACHIEVE): a multicentre, randomised controlled trial. Lancet. 2023;402(10404):786-797. doi:10.1016/S0140-6736(23)01406-X
- Williamson JD, Pajewski NM, Auchus AP, et al. Effect of intensive vs standard blood pressure control on probable dementia: a randomized clinical trial. JAMA. 2019;321(6):553-561. doi:10.1001/jama.2018.21442
- Edwards JD, Xu H, Clark DO, Guey LT, Ross LA, Unverzagt FW. Speed of processing training results in lower risk of dementia. Alzheimers Dement (NY). 2017;3(4):603-611. doi:10.1016/j.trci.2017.09.002
- Coe NB, Miller KEM, Sun C, et al. Impact of cognitive training on claims-based diagnosed dementia over 20 years: evidence from the ACTIVE study. Alzheimers Dement (NY). 2026;12(1):e70197. doi:10.1002/trc2.70197
- Sabia S, Fayosse A, Dumurgier J, et al. Association of sleep duration in middle and old age with incidence of dementia. Nat Commun. 2021;12(1):2289. doi:10.1038/s41467-021-22354-2
- Satizabal CL, Beiser AS, Chouraki V, Chêne G, Dufouil C, Seshadri S. Incidence of dementia over three decades in the Framingham Heart Study. N Engl J Med. 2016;374(6):523-532. doi:10.1056/NEJMoa1504327
- Iliff JJ, Wang M, Liao Y, et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid β. Sci Transl Med. 2012;4(147):147ra111. doi:10.1126/scitranslmed.3003748
- Xie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373-377. doi:10.1126/science.1241224
- Agarwal P, Leurgans SE, Agrawal S, et al. Association of Mediterranean-DASH Intervention for Neurodegenerative Delay and Mediterranean diets with Alzheimer disease pathology. Neurology. 2023;100(22):e2259-e2268. doi:10.1212/WNL.0000000000207176
- Barnes LL, Dhana K, Liu X, et al. Trial of the MIND diet for prevention of cognitive decline in older persons. N Engl J Med. 2023;389(7):602-611. doi:10.1056/NEJMoa2302368
A note on what this is and isn’t
This publication is for educational and informational purposes only. It is not medical advice. Reading it does not create a physician-patient relationship. The framework described here reflects population-level evidence. Individual situations vary considerably based on personal medical history, family history, genetics, and other factors. Decisions about your own health, including any consideration of the interventions described, should be made in partnership with your physician, who knows your specific situation. Nothing in this publication should be interpreted as a recommendation to start, stop, or modify any medical treatment without the guidance of a qualified healthcare professional.
